AN OVERVIEW OF HOW TO TREAT & UNLOCK THE TRIGGER FINGER PATHOLOGY AT MY SPORTS INJURY CLINIC BASED ON A CONSERVATIVE, PHYSIOTHERAPEUTIC APPROACH.
Has that ever happened to you, not to be able to freely move your finger as it feels like locked? Get to know what you might be coping with, let’s dive into it.
Trigger finger is a finger of the hand that remains fixed after being flexed, without being able to extend. It is deemed as an inflammatory condition, as in, this can be elicited by some particular circumstances such as hormonal factors, mechanical factors, and anatomical issues (V Vuillemin et la 2012). It should be noted that this sort of condition is also known as de Quervain tendinopathy, and stenosing tenosynovitis. On some occasions help is usually required of the other hand to be able to extend trigger finger.

Sometimes a click is heard when extending it, alongside with a perceptible popping and locking sensation (Sefora Codazza et la 2020), more frequently in the morning, when getting up.
It can affect one or several fingers, the most common being the little finger, the ring finger and the thumb, being the last one the highest incidence, followed by the ring finger of the dominant hand.
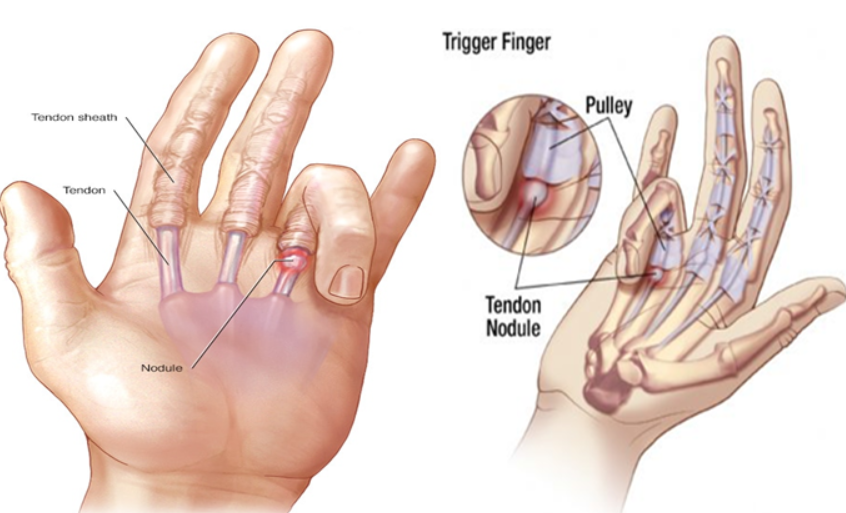
It is caused by an inflammation of the tendon sheath of the flexor tendons that generates an entrapment of these at the level of the pulleys of the fingers.
In the majority of the cases, it can be healed of its own accord, nonetheless, the trigger finger can also worsen bit by bit and get to a point where the locked finger in flexion cannot retrieve its mobility. This is why it is high-priority to regularly drop in your physiotherapist in Manchester at our Sports Massages Clinic Centre.
Therefore, you can be medical assessed and tackled by our physio specialists with their wealth of clinical experience, in both private and public systems. Our physiotherapist practitioners are contactable at My Sports Injury Clinic in the heart of Manchester City Centre and for the surrounding suburbs.
WHAT IS THE INCIDENCE OF TRIGGER FINGER? HOW COMMON IS TRIGGER DIGIT?
As much as, 3% up to 25% of sport-related injuries, are claimed to come about over the hands and the wrists. (YJ Lee et la 2021). According to study research performed to determining how common de Quervain tendinopathy is in professional bowling players, it reported that, this pathology was observed in 21 out of 39 subjects who were evaluated i.e., 53.8%.
On top of that, figures of 52.4 % and 42.9% of them had gotten pain and discomfort during and post training. It is stated based upon literature that this upper limb pathology is outstandingly high in people who often practice this sort of physical activity or hobby (IS Jamal-Azmi et la 2021).

In the same way, there was a report where this finger ailment was pinpointed in an adolescent who actively practice fencing, this was specifically spotted in his middle finger. Thus, this atypical situation in fencing players was firstly medicated with a splint, following anti-inflammatory medications (NSAIDs), and in the long run a steroid shot was necessary to ultimately eradicate the problem (Jonathan T W Au Eong et la 2021).

Trigger finger is more common after 40 years of age i.e., the 5th and 6th decade of life and it has been set out that is more frequent in women in comparison to men, women are 6 times more prone to sustain this finger condition than men. 2% to 3% of the worldwide population may present it at some point in their life. Albeit, chances might add up to 10% in patients with diabetes (Al Hasan Makkouk et la 2008).
WHAT ARE THE CAUSES OF TIRIGGER FINGER?
The causes of trigger digit are not clear enough. It is believed to be due to an inflammation of the tendons that join the wrist bones to the muscles of the fingers or an inflammation of a membrane that covers these tendons. People with jobs or activities that involve repetitive flexing and extension of the phalanges are prone to sustain it.
Its appearance is more frequent in people with certain diseases, such as rheumatoid arthritis, diabetes, renal disease, amyloidosis, hypothyroidismor carpal tunnel syndrome, or in people on dialysis (M Chammas et la 1995).
People who repeatedly use the muscles of the wrist or palm of the hand (for example, frequently screwing or unscrewing, holding something tightly for a long time). After the use of tools that compress and hit the muscles or tendons of the palm of the hand.
It can be seen more often in construction workers, industrial workers, farmers, and musicians. However, on many occasions it appears in people who until then were healthy without any reason that justifies it.
WHAT SYMPTOMS ARE PRODUCED BY TRIGGER FINGER?
Trigger finger causes difficulty stretching (extending) one or more fingers of the hand. This difficulty is usually accompanied by pain or swelling at the base of the finger. The difficulty is greater after a period of inactivity (for example, when you get up in the morning) and improves throughout the day, as you move more.
HOW CAN TRIGGER FINGER BE DIAGNOSED?
Trigger finger is a clinical diagnosis. In most cases, additional tests are not necessary for diagnosis. The standard characteristic of this trigger digit is the popping, locking, and clicking sensation which is superb helpful to provide confirmation of the trigger digit disease. Moreover, in the onset of the symptoms of trigger finger, it is visible pain and swelling in the flexor sheath of the affected finger.
Besides, our sports massage practitioners in Manchester will thoroughly inquire about existing pathologies that predispose to the development of trigger finger such as hypothyroidism or diabetes as this will be of great aid at verifying the diagnosis of trigger digit.
There is also another way to bear out the trigger digit diagnosis and this is the application of a lidocaine injection into the injured flexor sheath of the digit at issue, this ought to set the pain at ease.

In terms of imaging studies, there is no relevance in diagnosing for this kind of digit ailments. Due to it is deemed non-essential in patients who have not presented prior trauma, or inflammatory disease (Katzman BM et la 1999).
Apart from what has been claimed above, according to literature research the finding of a locking digit cannot be merely regarded as trigger finger as it might be as a result of dislocation, sesamoid bone anomalies, flexor tendon/sheath tumor, Dupuytren’s contracture, and focal dystonia, amongst others (Kalms SB et la 1991).
CAN TRIGGER FINGER BE PREVENTED? HOW IS THAT POSSIBLE?
Trigger finger can be prevented by avoiding actions that hit the tendons and muscles in the palm of the hand. Tenosynovitis can only be partially prevented. As a general rule, if the cause is an underlying disease (for example, rheumatoid arthritis) that causes the thickening of the tendon sheath of the fingers and produces the typical jerky movements of the fingers and pain in the affected finger of tenosynovitis, it will be necessary to treat this cause in time so that trigger finger does not develop.
It can also be caused by mechanical overloading of the finger tendons. Inappropriate and excessive movements should therefore be avoided and the muscles and tendons should be strengthened with regular finger exercises.
WHAT IS THE PROGNOSIS FOR THOSE WHO SUFFER FROM TRIGGER FINGER?
Trigger finger usually resolves in almost all cases after several weeks of treatment. The recovery of this injury depends on the approach taken, generally in a conservative treatment, in approximately 10 days the person could be resuming activities with light grip. However, recovery from the surgical approach takes more than 3 weeks, with the consequent risk of generating adhesions if an appropriate follow-up of the evolution is not carried out.
In this sense patients must be briefed not to precipitately resuming physical training/activities with the injured hand, also, they must be furthered to gradually return to sporting activities so further damaged can be staved off (Jeehae Oh et la 2015).
So, our physiotherapists in My Sports Injury will definitely recommend you not to rush your come back to your physical activity routine.
WHAT IS THE TREATMENT OF TRIGGER FINGER? CAN NON-SURGICAL TREATMENT HELP UNLOCK IT?
In many patients, trigger finger simply goes away with rest (sometimes a splint is placed to reduce finger mobility) and anti-inflammatories. When it is not cured with these measures, the following should be assessed.
Corticosteroid injection into the tendon sheath. They are usually injected with an anesthetic so that it does not hurt. They reduce inflammation in the area where they are administered. Many times, a splint is placed later to rest the finger for a few days. It fixes the problem in more than 9 out of 10 cases. Sometimes a second injection must be given. This method for tackling trigger digit is extremely effective and safe which reported an effectiveness rate of 79.7% according to a research study (Cornelius Schubert et la 2013).
A study by (Benan N Dala-Ali et la 2012) investigated the efficacy of corticosteroid injection in 90 trigger fingers, with a one-year follow-up. The authors managed to show a good effectiveness in 66% of the cases.

A retrospective review carried out by (Kristin Valdes in 2012) found an effectiveness rate of 87% in the treatment with trigger finger orthoses, without the need for new interventions during the year after the investigation was carried out.
According to the evidence, the use of orthoses also seems to be a useful treatment in the approach to trigger finger. A systematic review published in 2017 by Lunsford, Valdes and Hengy states that the continuous use of orthoses for a period of 6 to 10 weeks can achieve a clear decrease in trigger finger symptoms.
The effect of extracorporeal shock waves (ESWT) in this pathology has recently been investigated and some studies such as those published by Malliaropoulos et la in 2016, Yildirim et la in 2016, Dogru, Narin and Erduran in 2017 suggest that shock waves could be an effective treatment for trigger finger
Surgery, as in many other pathologies, is usually the last treatment resource and is used when the conservative approach has not been effective or when the severity of the trigger finger makes it necessary.
An investigation by (Sato et la 2012) where the debate on the most effective technique was kept open, since it compared the effectiveness of corticosteroid injection vs. surgical techniques, and in this study, surgery was found to be more effective than conservative treatment, although the authors affirm that the trigger digit should be treated conservatively first and surgical intervention should be used as a second option.
An operation under local anesthesia that opens the covering of the tendon to release it. It is usually curative in most cases. A percutaneous (unopened) operation can also be done using a needle.
SO, WHAT IS THE ROLE OF MY SPORTS INJURY CLINIC BASED IN MANCHESTER CITY IN TREATING TRIGGER FINGER?
Reading what the evidence says about the most effective treatments in this pathology could lead us to think that Physiotherapy in Manchester can do little in the patient with trigger finger, but in reality, this is not the case.
Physiotherapy plays a very important role in patient education, as well as in rehabilitation after surgery. Exercises to improve the flexibility of the soft tissues and maintain the functionality of the hand, fingers and adjacent joints, as well as scar treatment, are essential in post-surgery treatment. Some Physiotherapy tools are currently being studied, without definitive results.
It is interesting to mention that a recent study published in 2018 by McKee, Lalonde and Lalonde states that in 52% of patients trigger finger resolves spontaneously and in the thumb 72% of cases would resolve without treatment.
We must also point out that most of the studies presented have methodological limitations and, although they constitute a clinical guide, we must be aware of these limitations. Treatment should always be individualized and the patient's evolution will depend on many factors, including the degree of tendon entrapment and the thickening of the pulley or the tendon itself.
Although there is no magic formula that resolves trigger finger, a multidisciplinary management that takes into account the different resources supported by evidence will allow greater clinical improvement and a better functional result in the patient.
WHAT ARE THE BEST EXCERCISES TO GET BETTER MY TRIGGER FINGER?
Before these exercises, you can perform a massage of the affected joint, to facilitate blood flow and help lubricate it to prepare it for the exercises, gently rubbing the entire joint through circular movements for 2 or 3 minutes.
Place your hand with the affected finger on a flat surface and lift the affected finger as high as you can, holding the stretch in this position for 30 seconds. The exercise should be repeated 3-5 times.
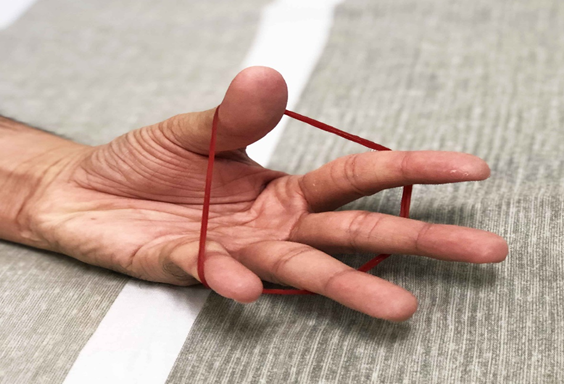
Place an elastic band around the fingers and then use the fingers to open the hand, stretching the elastic. Then slowly return to the starting position and repeat this exercise 10 to 15 times.
Place a modelling clay mass under your hand and try to stretch it, keeping your fingers straight, as shown in the image, repeating the same exercises for 2 minutes.
All exercises should be done slowly and when the person begins to feel pain they should stop. Also, to relieve hand stiffness, warm the tendons, and help stretch your finger, you can place your hand in a bowl of warm water.
Published by Rafael Peña for www.mysportsinjury.co.uk
REFERENCES
Vuillemin V, Guerini H, Bard H, Morvan G. Stenosing tenosynovitis. J Ultrasound. 2012 Feb;15(1):20-8. doi: 10.1016/j.jus.2012.02.002. Epub 2012 Mar 9. PMID: 23396894; PMCID: PMC3558240.
Ferrara PE, Codazza S, Maccauro G, Zirio G, Ferriero G, Ronconi G. Physical therapies for the conservative treatment of the trigger finger: a narrative review. Orthop Rev (Pavia). 2020 Jun 26;12(Suppl 1):8680. doi: 10.4081/or.2020.8680. PMID: 32913608; PMCID: PMC7459363.
Lee YJ, Harmony T, Jamal-Azmi IS, Gunasagaran J, Ahmad TS. Bowling: Occupational Hazards of the Wrist and Hand in Elite Tenpin Bowlers. Malays Orthop J. 2021 Mar;15(1):113-118. doi: 10.5704/MOJ.2103.017. PMID: 33880157; PMCID: PMC8043644.
Au Eong JTW, Sebastin SJ. Trigger Finger Associated with Fencing in an Adolescent: A Case Report. J Hand Surg Asian Pac Vol. 2021 Sep;26(3):463-466. doi: 10.1142/S2424835521720176. PMID: 34380406.
Makkouk AH, Oetgen ME, Swigart CR, Dodds SD. Trigger finger: etiology, evaluation, and treatment. Curr Rev Musculoskelet Med. 2008 Jun;1(2):92-6. doi: 10.1007/s12178-007-9012-1. PMID: 19468879; PMCID: PMC2684207.
Chammas M, Bousquet P, Renard E, et al. Dupuytren’s disease, carpal tunnel syndrome, trigger finger, and diabetes mellitus. J Hand Surg [Am] 1995;20:109–14. doi: 10.1016/S0363-5023(05)80068-1.
Katzman BM, Steinberg DR, Bozentka DJ, et al. Utility of obtaining radiographs in patients with trigger finger. Am J Orthop. 1999;28:703–5.
Kalms SB, Hojgaard AD. Trigger finger: report of an unusual case. J Trauma. 1991;31:582–3.
Oh J, Jo L, Lee JI. Do not rush to return to sports after trigger finger injection. Am J Phys Med Rehabil. 2015 Apr;94(4):e26-30. doi: 10.1097/PHM.0000000000000267. PMID: 25785923.
Schubert C, Hui-Chou HG, See AP, Deune EG. Corticosteroid injection therapy for trigger finger or thumb: a retrospective review of 577 digits. Hand (N Y). 2013 Dec;8(4):439-44. doi: 10.1007/s11552-013-9541-6. PMID: 24426963; PMCID: PMC3840755.
Dala-Ali BM, Nakhdjevani A, Lloyd MA, Schreuder FB. The efficacy of steroid injection in the treatment of trigger finger. Clin Orthop Surg. 2012 Dec;4(4):263-8. doi: 10.4055/cios.2012.4.4.263. Epub 2012 Nov 16. PMID: 23205235; PMCID: PMC3504690.
A Retrospective Review to Determine the Long-term Efficacy of Orthotic Devices for Trigger Finger. Valdes, Kristin. Journal of Hand Therapy, Volume 25, Issue 1, 89 – 96 DOI:https://doi.org/10.1016/j.jht.2011.09.005
Conservative management of trigger finger: A systematic review. Lunsford, Dianna et al. Journal of Hand Therapy, Volume 32, Issue 2, 212 - 221 DOI:https://doi.org/10.1016/j.jht.2017.10.016
Edson S. Sato, João B. Gomes dos Santos, João C. Belloti, Walter M. Albertoni, Flavio Faloppa, Treatment of trigger finger: randomized clinical trial comparing the methods of corticosteroid injection, percutaneous release and open surgery, Rheumatology, Volume 51, Issue 1, January 2012, Pages 93–99, https://doi.org/10.1093/rheumatology/ker315
Yildirim P, Gultekin A, Yildirim A, Karahan AY, Tok F. Extracorporeal shock wave therapy versus corticosteroid injection in the treatment of trigger finger: a randomized controlled study. J Hand Surg Eur Vol. 2016 Nov;41(9):977-983. doi: 10.1177/1753193415622733. Epub 2016 Sep 28. PMID: 26763271.
McKee D, Lalonde J, Lalonde D. How Many Trigger Fingers Resolve Spontaneously Without Any Treatment? Plast Surg (Oakv). 2018 Feb;26(1):52-54. doi: 10.1177/2292550317740691. Epub 2017 Nov 21. PMID: 29619360; PMCID: PMC5871113.