

PAIN AND NUMBNESS CAUSED BY NEUROPATHY IN THE UPPER EXTREMITIES
PAIN AND NUMBNESS CAUSED BY NEUROPATHY IN THE UPPER EXTREMITIES – KNOW ALL ABOUT THE PRONATOR TERES SYNDROME THE CARPAl TUNNEL SIMULATOR.
The Pronator Teres Syndrome (PTS) is a reasonably rare injury for which patients go to our team of competent physiotherapists with high expertise at our Sports Rehabilitation Centre known as My Sports Injury Clinic located in the city of Manchester, in which it is provided to each of our patients, whether elite athletes or businessmen, a comprehensive assessment and an accurate diagnosis to continue with the necessary treatment and rehabilitation programs implemented by our sports physios in Manchester to address and treat in the most appropriate way these types of injuries called nerve compression, also known as neuropathies in the upper limbs. In this case, we will elaborate on the pronator teres syndrome insight that is often confused with carpal tunnel syndrome. My Sports Injury Clinic Blog discusses the biomechanics, symptoms, anatomy, and different treatments of this condition carried out by the sports therapist practitioners. Also, it presents follow-up guidelines and shares some ideas on how sports physical therapists can deal with this rare injury.
Before explaining the injury and its entire approach, we must know what the anatomical structure known as the pronator teres consists of and its main functions.
What does the pronator teres consist of?
The pronator teres is a prominent muscle that belongs to the epitrochlear muscles and that crosses from the inner part of the elbow to the outer edge of the radius bone. Hence, it is due to the position it has that it can perform a rotational movement that involves the two bones of the forearm.
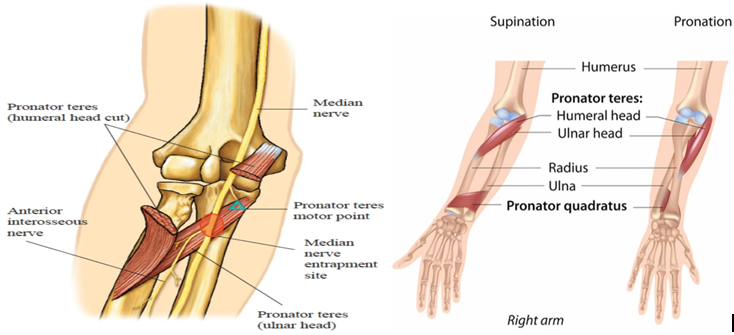
Muscles are found in many parts of the body, which is why they have different sizes and arrangements of their fibers. For example, in the forearm, the pronator teres and the pronator quadratus, the palmaris longus, the flexor carpi radialis longus, and the ulnar anterior are located on the anterior face.
What does the pronator teres do? – What movement does the pronator teres muscle perform?
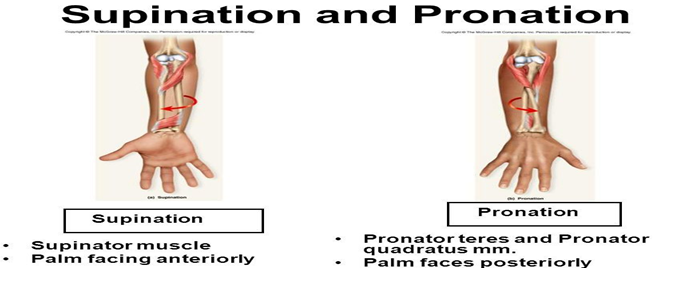
Thanks to the arrangement of its muscle fibers, it is a tissue capable of rotating the bones of the arm, which ends up bringing the thumb in a medial direction. This is known as pronation, supination being its opposite movement. Besides, some authors point out that he also flexes the elbow.
What injuries affect the pronator teres?
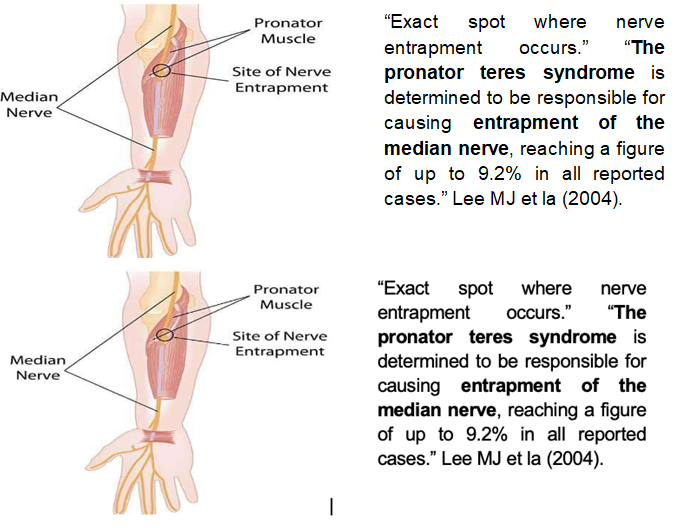
“Many injuries of muscular origin can affect the muscle ( tears, contusions, strains, etc.), but specifically there is one known as the pronator teres syndrome, which affects the median nerve with greater predominance as it passes through this place. Causing characteristic symptoms such as pain, loss of strength, and difficulty in moving the area.” Marine Dididze et la (2021).
What causes pronator teres syndrome?
Pronator Teres Syndrome broadly originates from reiterative motion, which causes a lot of tension in the muscles of the forearm. If your daily activities incorporate any activity that demands continuous rotation of the forearm muscles such as cleaning fish, repeated use of screwdrivers, and hammering those repetitive movements can lead to overuse of the muscle known as Pronator Teres.
“The causes of pronator teres syndrome may be related to trauma to the upper limb, with the formation of a hematoma or bone deformity, as well as congenital anomalies and due to hypertrophy of the pronator teres muscle and fascia. The presence of a mass, such as a lipoma, can also cause extrinsic pressure on the nerve. More cases in the literature have described the presence of a fibrous band between both heads of the pronator teres muscle, as the main compression site, and this leads to variable symptoms with limitation of function.” As stated by Jon A Jacobson et la (2010).

Graphic representation of forearm pain due to pronator teres syndrome | MYO shows you how to relieve it.
In which sports are you more likely to suffer from pronator teres syndrome?
Forearm aches due to pronator teres syndrome. This is an uncommon situation for elite athletes, whose exercise requires a firm grasp in the posture of forearm pronation, such as bodybuilders, tennis practitioners, baseball batters, cricket, and rowers. The symptoms can simulate be more like carpal tunnel syndrome which is more common.

A firm grip in pronation position by rowers.
Common symptoms and signs experienced by pronator teres syndrome athletes include:
- Aching discomfort (39%).
- Weakness (49%).
- Numbness (58%).
- Paresthesia (25%).
At My Sports Injury Clinic Rehabilitation Centre, we have undergone rigorous training to treat this condition. We are an interdisciplinary sports physiotherapy clinic in Manchester City, providing sports massages / deep tissue massage therapy, myofascial release, chiropractic, rehabilitation exercises, manual therapy, personal training, physical therapy, and acupuncture. Using these different types of services we can help the patients and the customers achieve the best results and best conditions to live pain and limitations free.
How can you treat pronator teres pain? – What is the conservative treatment for pronator teres syndrome?
“Some authors suggest a period of immobilization, although a regimen that includes movement and rest of the flexor muscles of the forearm, stretching exercises, mild activity, modification of the activity that produces pain for a minimum of six months has been more recommended, accompanied treatment with anti-inflammatory drugs.” Mackinnon and Novak (2011)
“Other authors comment that in a patient with arm pain with occasional paresthesia, supportive measures are recommended, such as analgesics, periods of ice / heat, rest splint, and activity modification. And they also cite that, without the necessary evidence to support the efficacy of surgical decompression of the median nerve in patients with scattered symptoms in pronator syndrome. They are in favor of conservative treatment.” Norris et la (1976).
“Conservative treatment is effective in 50% to 70% of patients. Corticosteroids have also been shown to be effective. Morris and Peters found that corticosteroid therapy in the pronator teres, combined with activity modification, resulted in a subjective improvement of symptoms in five of the seven patients studied.”
“The implementation of electrical stimulation and ultrasound has been displayed to be beneficial in the treatment process of other neuropathies, and their implementation may be favorable in the pronator teres syndrome’s treatment. A study showed that 50% of pronator syndrome patients informed relief of symptoms within four months of starting care.” LaTayo et la (2004).
Is surgical treatment effective?
“When an occupying injury is present and conservative management fails, surgery may be indicated. The success rate with surgery in the treatment of pronator syndrome is close to 90% in the literature, although there is no consensus on how long a conservative treatment should be followed before surgical intervention.”
How is pronator teres syndrome diagnosed? – How do you test for pronator teres syndrome?
The convalescent individual stands with an elbow flexed at 90 degrees. Then, the sports clinician/ physiotherapy practitioner is going to place one hand on the patient’s elbow to stabilise it, and the other one will hold the hand in the handshake position of the individual in pain. When the practitioner tries to turn into a supination position on the patient’s forearm, the patient will maintain this position, causing the patient to contract the muscles of the forearm.

While maintaining resistance to internal rotation, the clinician will stretch the patient’s elbow. If the discomfort or the pain of the patient reappears there is the possibility of the existence of compression of the median nerve by the pronator teres i.e. pronation activity exacerbates symptoms.
How is Pronator Teres syndrome treated? – How to strengthen the pronator teres.
Possibly the most significant aspect of the treatment process is to avoid reiterative strong grasps.
Determined massage techniques can help to ease the tenseness of your injured forearm in this way reducing your median nerve compression. These techniques can lengthen the pronator teres muscle and they are known as “releasing” the pronator teres, these types of sports massages must be carried out by sports physiotherapy clinicians. Even though upper limb exercises can relieve symptoms once they have been started, regular stretching exercises can also help control and possibly prevent PTS.

- Pronator teres stretching.

When bending your elbows, hold a heavy object (5-10kg) with your hand. Place heavy objects so that most of the heavy objects face the thumb side. Keep stretching for 30 seconds each time and repeat five times.
“EXERCISES ROUTINE TO STRENGTHENING THE PRONATOR TERES”.
- Strength exercises routine to focus on supinator teres.
For the disequilibrium between the supinator and the pronator teres, direct supination intensity work is required:
- Grab a weighted stick or a hammer with just one hand.
- Maintain the elbow straight, so that one end of the counterweight turns the arm into an internal rotation position (this makes the supinator eccentric).
- Put back the stick or the hammer to the vertical position.
- Execute three series of fifteen repetitions.

REFERENCES
- Jacobson JA, Fessell DP, Lobo Lda G, Yang LJ. Entrapment neuropathies I: upper limb (carpal tunnel excluded). Semin Musculoskelet Radiol. 2010 Nov;14(5):473-86. doi: 10.1055/s-0030-1268068. Epub 2010 Nov 11. PMID: 21072726.
- Lee MJ, LaStayo PC. Pronator Syndrome and Other Nerve Compressions That Mimic Carpal Tunnel Syndrome. J Orthop Sport Phys Ther 2004;34:601-609.
- Gessini L, Jandolo B, Pietrangeli A. Entrapment neuropathies of the median nerve at and above the elbow. Surg Neurol. 1983;19:112-116.
- Hartz, C R, R L Linscheid, R R Gramse, and J R Daube. “The pronator teres syndrome: compressive neuropathy of the median nerve.” The Journal of Bone and Joint Surgery. American Volume 63, no. 6 (July 1981): 885-90.
- Morris, H H, and B H Peters. “Pronator syndrome: clinical and electrophysiological features in seven cases.” Journal of Neurology, Neurosurgery, and Psychiatry 39, no. 5 (May 1976): 461-4.
- Eversmann WW. Proximal median nerve compression. Hand Clin. 1992;8:307-315.
- Nebot-Cegarra J, Perez-Berruezo J, Reina de la Torre F. Variations of the pronator teres muscle: predispositional role to median nerve entrapment. Arch Anat Histol Embryol. 1991;74:35-45.
- Tulwa N, Limb D, Brown RF. Median nerve compres- sion within the humeral head of pronator teres. J Hand Surg [Br]. 1994;19:709-710.
- Howard FM. Compression neuropathies in the anterior forearm. Hand Clin. 1986;2:737-745.
- Institute for Integrative Healthcare Studies; Techniques for Releasing the Pronator Teres; N. Cutler, L.Ac.; October 2009