

Rehabilitation After Surgery: Physical therapy for Spine Stenosis Disorder
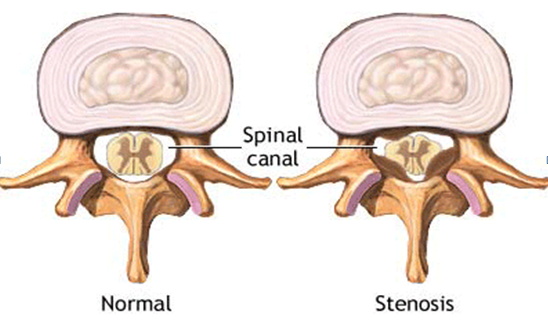
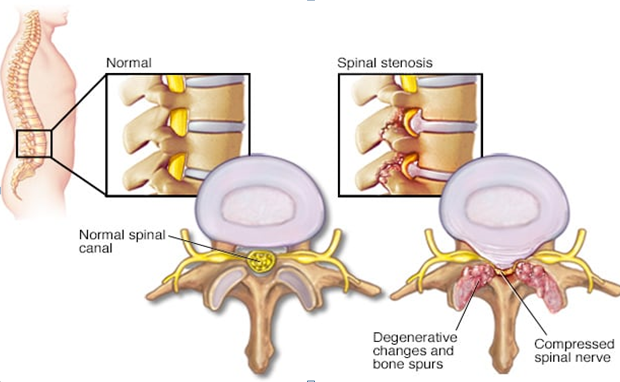
What are spinal stenosis disorders of the spine? Spinal stenosis is a common condition that occurs when the spinal canal, which contains the nerve roots and spinal cord, becomes compressed. This causes a “stinger” of the nerve roots and spinal cord, resulting in pain, cramps, weakness, or numbness. Depending on where the narrowing occurs, these symptoms may be felt in the lower back and legs, buttocks, neck, shoulders, or arms (Avais Raja et la, 2021).

Anyone over the age of 50 is vulnerable to sustain it although this spinal disorder known as spinal stenosis is also the main reason of spinal surgery in patients who are aged over 65 years. Lumbar spinal stenosis is a determining factor of disability within elderly population (Lite Wu et la, 2021). Even more unusual, lumbar spinal stenosis may be secondary to congenital causes such as achondroplasia. The narrowing is usually brought about by osteoarthritis (or “wear and tear” arthritis) of the spine and the discs between the vertebrae.
IS PHYSICAL THERAPY GOOD FOR SPINAL STENOSIS?
Sports physical therapy is paramount when creating a treatment plan to dealing with spinal stenosis since through spine disorders pain exercises that being carried out during rehab session, patients can strengthen their muscles of the lower back and bring back mobility, explained by VerywellHealth. Spinal disorders back pain exercises and physical therapy Manchester is of great importance in the treatment of this disorder. Regular exercise to keep muscles strong and improve flexibility increases strength, decreases pain and improves general well-being. Treatment selection will be based on how severely spinal stenosis symptoms affect your quality of life and daily activities.
Physical therapy for spinal stenosis includes treatments with mechanical or physical means, such as exercise routine or heat. Physical therapy Manchester can diminish soft tissue pain (such as ligaments, tendons, and muscles), targeted to increase muscle strength, and improve performance/function, according to the medical journal University of Michigan State.
The biomechanics of the lumbar spine produces changes in the diameter of the medullary canal depending on the position of our lumbar spine. Thus, during the flexion movement of the trunk, this channel increases its diameter and during the extension movement it decreases. The approach to this type of pathology from the point of view of physiotherapy must include techniques and exercises that favour the movement of lumbar flexion, facilitating the increase in the diameter of the spinal canal.
On the other hand, work must be done to prevent lumbar flexion from causing the appearance of other symptoms and to improve the general physical condition of the patient.
For this reason, sports rehabilitation should focus on performing mobilisations and lumbar flexion exercises by both the physiotherapist Manchester and the patient, such as work in pelvic retroversion, bring the knees to the chest in the supine position, both simultaneously and alternately, quadruped lumbar flexion, and in a sitting position, bend over with your hands between your legs. As well as, neuromuscular electrical stimulation is the gold standard treatment after spinal cord injury as it prevents the involved musculoskeletal structures to be harmed (David J. Arpin et la, 2019).
This should be combined with cardiovascular work, strength and elasticity of the lower limbs, and posture aimed at avoiding hyperextension postures.
According to an article by ClevelandClinic, if you present any other spinal disorder condition such as scoliosis, herniated disc, you might be highly prone to developing spinal stenosis as well.
On the other hand, there is a close causal relationship between cervical cord neuropraxia and cervical spine stenosis as they are quite alike spine disorders in grown-ups, this appreciation has not been noticed in children. Therefore, the prevalence of this disorder in athletes and sporting events is 1.3-6 per 10.000 athletes; nonetheless, there is lack of literature discussing this subject (Aaron J et la, 2011).
IS SURGERY THE BEST OPTION FOR SPINAL STENOSIS DISORDER?
Several recent studies have shown that surgery produces better results than non-surgical treatment in the short term. However, results vary, and like all surgeries, this one also carries risks. Some of these risks are; blood clots in the brain or legs, tears in the tissue around the spinal cord, infection, and nerve root damage. Although surgery may provide some relief, it will not cure spinal stenosis or osteoarthritis, and symptoms may return, this procedure is called laminectomy (Ian A Harri et la, 2016).
HOW IS SPINAL DISORDER DIAGNOSED?
A doctor/ sports clinician or sports physiotherapist Manchester will ask about your symptoms and medical history. If you suspect spinal stenosis, you will have a clinical physical exam. Some of the symptoms that the physiotherapy Manchester specialist will look for are.
Numbness, weakness, cramps, or pain in the legs, thighs, and feet that makes it hard to walk, pain down the leg, abnormal bowel and/or kidney function, loss of sexual function.
Partial or complete paralysis of the legs can occur in severe cases; this is considered a medical emergency and you should go to an emergency room as soon as possible.
The medical care provider will also consider other conditions that can cause similar symptoms, such as arthritis of the hips or knees, disorders of the nervous system, heart, and blood vessels. Physical therapist may also order other tests to confirm the diagnosis and determine the severity of your condition. Amongst them are the following.
An x-ray of the spine to check for osteoarthritis, bone spurs, and a narrowing of the spinal canal, a computed tomography (CT) scan, which takes detailed pictures of your back and spinal canal, an MRI of the spine to take pictures of the spinal cord and nerves, an electromyogram (EMG) to check the nerves going to the legs, X-rays of the hips or knees, blood tests, as well as tests to check circulation in the legs and to rule out other conditions with similar symptoms (João Levy Melancia et la, 2014).
HOW TO KNOW IF YOUR BACK AND SPINE IS AFFECTED IN EARLY STAGES
Most cases of spine and back pain are caused by conditions of the spinal structures. Depending on the cause, spine or back pain may be accompanied by neurological symptoms (Peter J. Moley, 2020).
If a nerve root is affected, the pain may radiate distally along the distribution of the nerve root (radicular pain). Strength, sensation, and reflexes in the area innervated by this root may be impaired.
If the cauda equina is affected, a segmental deficit develops in the lumbosacral region, typically with compromised bowel function (constipation or fecal incontinence) and bladder function (urinary retention or incontinence), loss of perineal sensation, erectile dysfunction, and loss of rectal tone and sphincter reflexes.
Any painful condition of the spinal cord can also cause a reflex spasm of the paraspinal muscles.
Practical Advice for Recovering from Back Surgery. If in Pain, Ask for help!
Post-Op surgery can be very daunting especially if not pre -planned. Taking time to recover is imperative to improving the physical health and well-being of an individual.
The physician and nursing staff will provide instructions for pain medication and a written discharge alongside physical therapy and Exercise rehabilitation.
Oral pain management analgesic drugs are commonly prescribed for pain relief post-op however it should be noted that unpleasant side effects can result including respiratory disorders, depression, nausea, and vomiting.
Post-operative pain can initiate symptoms including pain receptive response, neuropathic and inflammatory type pains from tissues such as the vertebrae, spine disc, ligaments or joint capsules (Mathiesen O, et al 2013).

Stretching Regularly through the day
Dependant on the mobility of the joint Post-Op gentle stretching should be considered. Continuous movements help to circulate blood bringing valuable nutrients to the site of injury. Patients should be made aware of their limitations and activity restrictions following surgery to avoid anything too intense or exacerbating to the injured area. (Restrictions i.e bending , twisting, lifting) and specific activities should be pursued or avoided (i.e biking, walking, swimming, etc).
WHEN SHOULD PATIENTS START PHYSICAL THERAPY TREATMENT POST SURGERY?
Conservative Physical or Manual therapy treatment was appropriate considered for patients without clear abnormalities and for those with new pain differing from the original symptoms. Neuro-stimulation was considered appropriate in the case of neuropathic leg pain in the absence of conditions that may require surgical intervention.
Re-operation could be considered for patients with recurrent disc, spinal/foraminal stenosis, or spinal instability (Tronnier et al, 2018).
Seeing a sports physiotherapist can be beneficial using Transcutaneous electrical nerve stimulation (TENS) can be an efficient method for providing analgesic relief pot-operatively reducing opioid treatment (Unterrainer AF, et al 2012).
Initial appointment bookings can be made by visiting MY Sports Injury Physical Therapy and Rehabilitation Clinic in Manchester City
MY Sports Injury Clinic, we offer comprehensive and specialised care; our focuses are movement as a main outcome to recover, to maintain optimal quality of life and re-establish activities of daily living. Our professional practitioners have a depth of knowledge expertise, and experience in providing a high quality standard of care.
At MY Sports Injury Clinic | Manchester we also provide an holistic approach using effective, safe treatment techniques and advanced technology, seeking to shorten rehabilitation times and prolong functional movement, overall health and longevity.
Some of the specialist treatments services we carry out are Sports physical therapy, Medical Acupuncture, Sports massages, Manchester Deep tissue massage, and Sports injury rehabilitation amongst others. The most frequent pathological conditions / Injuries that our Sports Injury Specialists handle at My Sports Injury Clinic are musculoskeletal injuries, fractures, sprains, myalgia, dislocations, pre and post-operative, overuse injuries, postural disorders, muscle imbalances and Pain management.
WHAT ACTIVITIES SHOULD BE AVOIDED WITH SPINAL STENOSIS?
3 Spinal Stenosis Exercises To Avoid
- Avoid stretching in a standing position and extension stretches. Instead, try stretching while laying down.
- Avoid doing free weights. Instead, try using a weight machine.
- Avoid running and similar high-impact exercises. Instead, try swimming, cycling, or an elliptical machine.

SHOULD WE USE ANY ERGONOMIC SUPPORTS TO CORRECT POSTURE FOR BACK SUPPORT?
The use of Ergonomic Supports
Such as foot stools, chairs, and orthopaedic sit-to-stand desks can be beneficial to avoid placing excessive joint pressure or strain on the injured structures in the back. Ergonomic lumbar chair supports can help keep the spine in proper spinal alignment.
Avoid prolonged sitting and take active breaks between work
This can place additional strain on the lower back as its difficult for most people to maintain a healthy sitting posture when sat long periods of time. Prolonged sitting becomes uncomfortable the body tends to slouch and cause mis-alignment, or changes in position disrupting good ergonomic posture.

Achieving a healthy weight.
Post-Surgery can be beneficial as it places less stress and strain on the structures in the spine reducing spinal disc pressure which will further minimize loading of pressure and symptoms in the lower back.
Eating Nutritionally.
By Eating nutrient dense sources of food will nourish and fuel the body to enhance the repair process of healing. Patients should ask their doctor or nutritionist of any implications of post-surgical pain medication that they should be aware of. (I.e, Pain medications, non-steroid anti-inflammatory drugs as some can cause side effects leading to constipation. Eating plenty of nutritious foods with a high fibre content is important.
RISK FACTORS TO CONSIDER POST-OPEARATION
Postoperative spine infection can have devastating complication after spinal surgery in both the short term and long term. Infection places a patient at a high risk for pseudoarthrosis, chronic pain, return to operating room, adverse neurological consequences, worsened long-term outcomes (Grauer et al, 2003).
Depending on the type of Operation specific signs nad symptoms of swelling could be present. Neurolgoical deficits, Abnormal subcutaneous skin i.e fatty skin development, loss of motor strength and control, sensation, or bladder & bowel changes).
Keeping an achievable pain control plan following surgery and discussing it with the patient so that realistic expectations are set in place about the type and level of pain can go a long way in improving the comfort and satisfaction of the patients.
WHAT IS CONSIDERED SEVERE SPINAL STENOSIS?
When stenosis develops itself to a severe stage it fundamentally means that spine has been going through substantial narrowing of the spinal canal, explained by Advanced Spine & Orthopedics.
DOES SPINAL STENOSIS AFFECT BOTH LEGS?
It does indeed; the pain usually affects both legs. Patients can walk greater distances without pain when supported on a cart and can also pedal a bicycle without pain, all due to the forward flexed position that improves the obstruction of the medullary canal.
Published by Rafael Peña for www.mysportsinnjury.co.uk
REFERENCES
Postoperative wound infections of the spine.
Beiner JM, Grauer J, Kwon BK, Vaccaro AR
Neurosurg Focus. 2003 Sep 15; 15(3):E14.
The appropriate management of persisting pain after spine surgery: a European panel study with recommendations based on the RAND/UCLA method
V Tronnier, S Eldabe, J Franke, F Huygen, P Rigoard, J de Andres Ares, R Assaker, A Gomez-Rice, M La Grua, M Moens, L Moke, C Perruchoud, N Quraishi, D Rothenfluh, P Tabatabaei, K Van Boxem, C Vleggeert-Lankamp, B Zoëga, H Stoevelaar, 2018
A comprehensive multimodal pain treatment reduces opioid consumption after multilevel spine surgery. Mathiesen O, Dahl B, Thomsen BA, Kitter B, Sonne N, Dahl JB, Kehlet H
Eur Spine J. 2013 Sep; 22(9):2089-96.
Raja A, Hoang S, Patel P, et al. Spinal Stenosis. [Updated 2021 Dec 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441989/
Wu L, Cruz R. Lumbar Spinal Stenosis. [Updated 2021 Aug 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531493/
Melancia JL, Francisco AF, Antunes JL. Spinal stenosis. Handb Clin Neurol. 2014;119:541-9. doi: 10.1016/B978-0-7020-4086-3.00035-7. PMID: 24365318.
Arpin David J., Ugiliweneza Beatrice, Forrest Gail, Harkema Susan J., Rejc Enrico. Optimizing Neuromuscular Electrical Stimulation Pulse Width and Amplitude to Promote Central Activation in Individuals With Severe Spinal Cord Injury; Frontiers in Physiology 2019; 10. 10.3389/fphys.2019.01310