

Scapulohumeral Rhythm, GIRD, and Dyskinesia: How to Improve Shoulder Function.
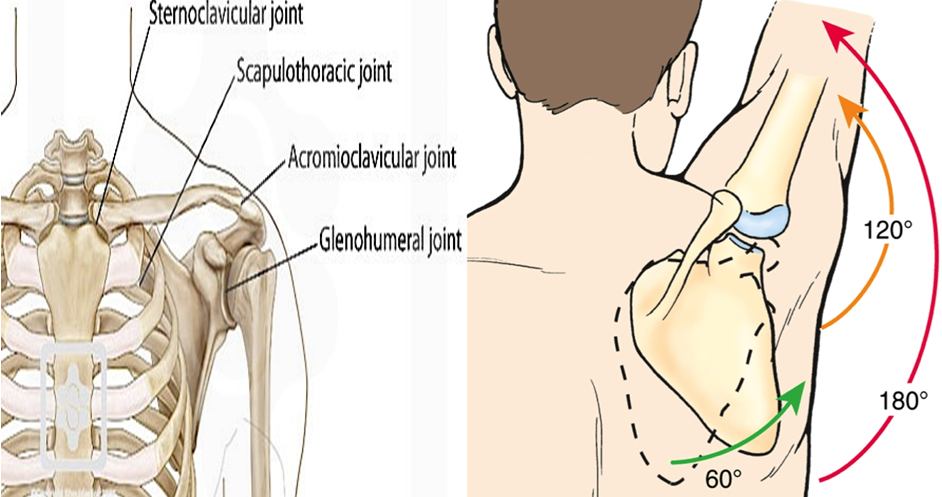
The coordinated movement between the glenohumeral joint and the thoracic scapula is known as the scapular humeral rhythm. When flexo-abduction of the shoulder is performed at 180 °, this movement immediately intervenes in the displacement of the scapula because this singular bone piece is an important part in stabilising the upper limb; of the 180 ° mentioned above, 120 ° have occurred in the glenohumeral joint while 60 ° have occurred in the scapulo-thoracic joint, which is known as the Scapulo-Humeral Rhythm.
“The impact of sporting-related practices on the scapular resting position and the scapulohumeral rhythm and its quantitative relation 75 subjects were included in this research that they were fifteen volleyball practitioners, fifteen table tennis practitioners, fifteen handball athletes, and fifteen non-sports individuals. It was found that the static position of the scapular bone between the main and non-main shoulders of each group did not have asymmetry in upward/downward rotation, but the main shoulder of the handball player had a larger downward ratio than the main shoulder of the non-athlete in the resting position. Besides, in the five groups, the shoulder-brachial rhythm ratios of different abduction angles are significantly different, because the scapular kinematic behavior ratio of table tennis players and non-athletes is larger than handball players. To summing up, even though, some healthy athletes from different sports and non-athletes may not have asymmetry in the up/down rotation, exercise-related activities may affect the scapulohumeral rhythm” By Seyed Hossein Hosseinimehr (2020).
The interrelatedness of these structures is essential for ideal mobility of the shoulders when the regular location of scapular bone relative to the humerus changes. It may lead to scapulohumeral rhythm dysfunction. Changes in the regular position are also called scapular dyskinesia.
“In this sense, the proposed ratio for this scapular humeral rhythm, according to Inman et la (1994), is 2: 1, that is, for every 3 degrees that occur in shoulder elevation, the second occurs at the expense of the joint glenohumeral and 1st by the action of scapular rotation.”
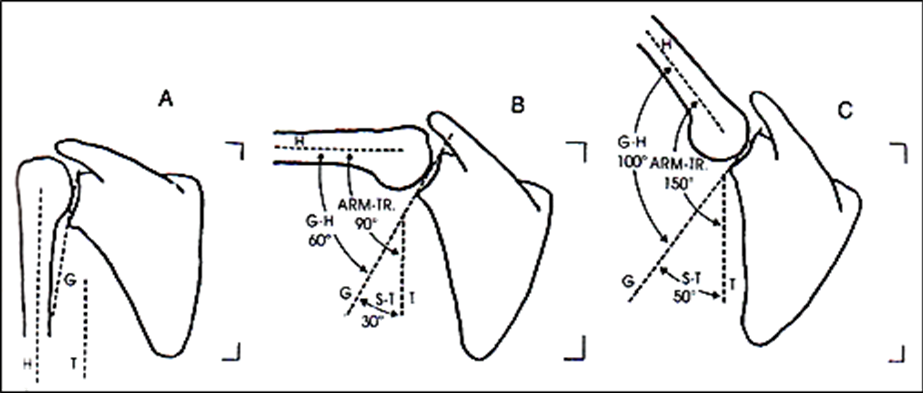
The lifting movement of the arm is carried out in a continuous, coordinated manner, during which for every 15º of movement, 10º lie in the glenohumeral and 5º in the scapular rotation, maintaining a ratio of 2: 1.
What is dyskinesia /scapular dyskinesia according to My Sports Injury Clinic Clinicians?
First of all, we must know that our physical therapists of MY SPORTS INJURY IN MANCHESTER CITY CLINIC CENTRE will explain to you that dyskinesia is abnormal involuntary movements that mainly affect the limbs, trunk, or jaw and that occur as a manifestation of an underlying pathological process.
According to the experts of MY SPORTS INJURY CLINIC, scapular dyskinesia is described as observable alterations in the position and movement of the scapula concerning the rib cage, which can generate alterations in the kinematics of the scapulohumeral, that is, this scapular dyskinesia most likely generates consequences in the gleno-humeral joint due to their intimate relationship in the movement.

Why does dyskinesia occur?
“Compared with non-overhead athletes, the prevalence of scapular dyskinesia in overhead athletes is higher, about 61% within sports like baseball, volleyball, basketball, American football, and cricket”.
Under Yamaguchi and Cols (2000) “There are several factors that can cause this alteration/ shoulder-scapula limitations. The most frequently encountered are Postural alterations that promote this pathology, such as in a resting position with excessive thoracic kyphosis and an increase in cervical lordosis, which can result in excessive scapular protraction and acromial depression, which increases the potential to produce impingement”.
Other factors associated with scapular dyskinesia stem from muscle dysfunction, specifically an alteration in muscle coordination. “For scapular stabilisation, co-contraction of the upper and lower trapezius and rhomboids with serratus anterior is required. For scapular elevation, co-contraction of the serratus anterior and lower trapezius with upper trapezius and rhomboids is required. If these muscular couplings do not occur, the production of scapular dyskinesis is possible. In the serratus anterior muscle, a decrease in its activity has been demonstrated in patients with subacromial impingement during loads and their phases” Ludewig and Cook (2000).
What are the different types of Dyskinesis that you could suffer from?
- Inferior dysfunction.
- Medial dysfunction.
- Superior dysfunction.
Another limitation of shoulder/scapular movement discussed in this article is GIRD (Glenohumeral Internal Rotation Deficit) which will be described below.
Are you ready for an appointment at My Sports Injury Clinic Rehabilitation Centre?
In MY SPORTS INJURY CLINIC located in Manchester City, we offer a huge variety of high ends rehabilitation programs focused on the well-being of the patient, and life without limitations.
How can be defined GIRD?
GIRD can be defined as the loss of degrees of glenohumeral internal rotation. This limitation tends to occur more frequently in pitchers of cricket and baseball, especially in the throwing shoulder compared to the non-throwing shoulder.

Loss of glenohumeral internal rotation on the skillful side compared to the other limb. This is a characteristic alteration of overhead sports.
“The main content of non-surgical treatment of GIRD patients is still posterior capsule stretching. A comprehensive treatment plan should also focus on the entire dynamic chain, including the lower limbs, core, and shoulder bones. For symptomatic throwers who cannot undergo extensive non-surgical treatment, shoulder arthroscopy can be performed. It is important to realise that not all patients with GIRD can be diagnosed with internal impingement.” Michael B Rose and Thomas Noonan (2018).
To conclude this article we share some conclusions:
- A retraction of the posterior capsule could be a risk factor for developing rotator cuff friction syndromes.
- Dysfunction of the scapulohumeral rhythm, either due to poor location, or an altered scapular movement, can result in a dysfunction in the scapulohumeral joint and the consequent increase in the risk of injury
What has been developed so far can serve as a starting point in the analysis of possible treatment approaches for impingement injuries or subacromial friction syndrome. This represents the irritation and wear generated by friction in the structures below the acromion and related to them.
References
- Kibler WB, Kuhn JE, Wilk K, et al. The disabled throwing shoulder: spectrum of pathology – 10-year update. Arthroscopy. 2013;29(1):141–161. e126.
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology – part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19(4):404–420.
- Kibler WB, Sciascia A, Thomas SJ. Glenohumeral internal rotation deficit: pathogenesis and response to acute throwing. Sports Med Arthrosc Rev. 2012;20(1):34–38.
- Ken Yamaguchiand col. Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. Journal of Shoulder and Elbow Surgery Volume 9, Issue 1, January–February 2000.
- Paula M Ludewig and Thomas M Cook. Alterations in Shoulder Kinematics and Associated Muscle Activity in People With Symptoms of Shoulder Impingement. Physical Therapy March 2000.
- Struyf, F., Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability, Scandinavian Journal of Medicine and Science in sports, jrg20, nr3, 2011, p352.
- Rundquist P, Anderson DD, Guanche CA, et al. Shoulder kinematics in subjects with frozen shoulder. Arch Phys Med Rehabil 2003; 84:1473–1479.
- Codman EA: The Shoulder,Boston: G.Miller & Company,1934.
- Hosseinimehr, Seyed Hossein & Anbarian, Mehrdad. (2020). The effects of activities related to sports on scapular resting position and scapulohumeral rhythm ratio. Sport Sciences for Health. 16. 10.1007/s11332-020-00647-1.